
Consider “quality:” every hospital touts its quality, every physician confidently affirms their delivery of high quality care, and every trade and professional sector in healthcare has its own definition that aligns with attributes of quality they deem most important. “Quality” is touted on every website and in every boardroom, but rarely is it defined and measured consistently.
“Outcomes” is another. Most ascribe positive outcomes in their performance, but the indicators on which they’re based and the time periods over which they’re captured—days, weeks, months, or years—varies from user to user. Valid and reliable measures are ephemeral: process measures are used more frequently because they’re easier for regulators, policymakers and payers to monitor; i.e. “advising a patient to stop smoking or lose weight” but these may have little to do with the actual outcome.
“Cost” is a third example of these elusive but widely used terms. It seems simple enough, but not so fast. When used by some, it’s inclusive of only direct costs that can be easily captured in the supply chain, like parts, drugs, disposables; or things easy to count, like length of stay, prescriptions or the number of calls run through a call center. But “costs” get tricky when corporate overhead, R&D and fixed costs are included, and rarely is the public given access to their formula. It’s ironic, then, that a standard definition of cost remains elusive in an industry that’s under such intense cost-reduction pressure.
And there are others: “population health management” is bantered widely but which population is being managed and what processes are deployed vary widely. Nonetheless, every health plan and health system is now in the population health management business. And “disruptive innovation” is another: though its finer points are a vigorous debate in academia these days, it is standard business-speak across the healthcare industry as insiders describe the efforts of outsiders and upstarts.
But the granddaddy of them all is “value.” Futurists are forecasting a colossal shift in payments “from volume to value.” Drug manufacturers are defending escalating drug costs on the basis of their value; i.e. their efficacy and effectiveness in treating a condition. Insurers are pushing the shift of financial risk to providers to accelerate the volume-to-value transition, and Medicare is promoting value-based purchasing in its alternative payments program.
But like “quality,” “outcomes,” “costs,” “population health” and “disruptive innovation,” “value” is not understood nor is a common definition widely accepted across the industry, and more important, outside. A classic definition for healthcare (a la Michael Porter) would be the outcomes received per dollar spent (1). But the healthcare industry has struggled to address value beyond broad conceptual frameworks and theoretic models. Reputable organizations and associations like those sampled below offer their unique approaches: most of these are based on expert judgment; a few are associated with empirical studies that correlate attributes with a measurable outcome. Some of the better known approaches to defining value are these:
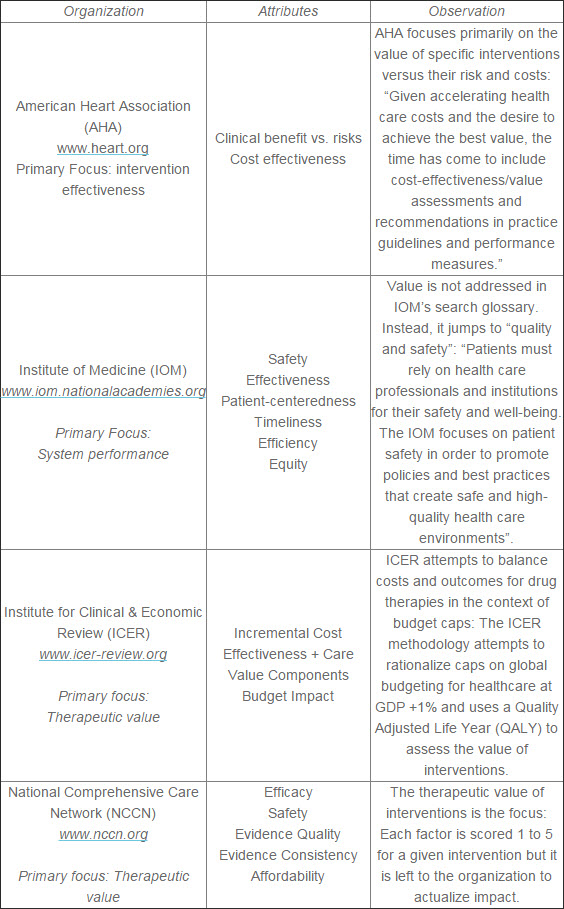
I spent time on each of these sites this weekend attempting to understand how the organization defines value. Most contextualize “value” as measure of the therapeutic value of an intervention. Most assume the value creator is the clinician and care team responsible for making clinical judgments. And all are paying more attention to value, though surprisingly, on a venerable and widely respected source like the Institute of Medicine. My search for “value” pointed me to “quality and safety” and there was no resource for its view of “value.”
As I reflect, in healthcare, we are more comfortable using an assembly line model to capture attributes and measures of value; i.e. value is the sum of component parts plus labor plus overhead divided by price. What people pay is obfuscated by our pluralistic payment system, and value is not consistently measured as a result.
What’s missing in this view is an understanding of value as defined by end users: patients, members, users (or more appropriately consumers). Arguably, they are industry’s most important constituent.As I reflect, in healthcare, we are more comfortable using an assembly line model to capture attributes and measures of value; i.e. value is the sum of component parts plus labor plus overhead divided by price. What people pay is obfuscated by our pluralistic payment system, and value is not consistently measured as a result.I spent time on each of these sites this weekend attempting to understand how the organization defines value. Most contextualize “value” as measure of the therapeutic value of an intervention. Most assume the value creator is the clinician and care team responsible for making clinical judgments. And all are paying more attention to value, though surprisingly, on a venerable and widely respected source like the Institute of Medicine. My search for “value” pointed me to “quality and safety” and there was no resource for its view of “value.”
In most industries, “value” as defined by consumers is associated with in four attributes:
- Accessibility: “can I get what I need or want from you?”
- Service: “is dealing with you a pleasant experience?”
- Effectiveness: “is what you’re providing going to satisfy my need or want?”
- Costs: “what’s the cost to me and my family and is it worth it?”
Simple enough. Pretty straightforward. Regrettably, the healthcare system from top to bottom routinely fails to address value to consumers along these same dimensions. We have many excuses—insurance coverage hassles, declining reimbursements, regulation and more. But they’re excuses. Academicians are vexing over the struggle to incorporate costs into the value debate in healthcare; drug and device manufacturers are promoting their proprietary methods of measuring value, insurers are arguing theirs is the only domain where value has been a serious pursuit, and providers are struggling to rationalize efforts targeting consumer value with traditional structures that reward cost effective manufacturing on a one size fits all chassis. (2, 3)
What would happen if a partnership of physicians, hospitals and insurers developed a system that’s solely built around a consumer’s definition of value? What if, instead of an assembly line, healthcare became a system of health that delivers high value to consumers?
Technologies that enable access to medical records, scheduling, prescription fulfillment and other routine services would be readily available. Hiding behind HIPAA as an excuse for shunning digital health would be a thing of the past.
Knowing what a test, procedure, drug or visit costs before it’s used would be SOP—delivered through the consumer’s smart phone and with comparison pricing readily accessible.
Having the processes and programs in place to accurately, and with compassion, explain the costs and complications and engage individuals and their families in end of life care discussion would take on added significance.
And the needs and preferences of consumers, stratified into cohorts by meaningful psycho-social-demographic variables would be factored into our programs and services in addition to signs, symptoms, risk factors and co-morbidities. The fire-walls between physical and mental health, allopathic and alternative methods of treatment, health and human services programs, access to providers and investments in community health, primary care and specialty care and others would quickly be torn down.
For all the chest thumping we do about the performance of our health system, you’d think value as defined by our most important constituents—consumers—would be more important to us. Perhaps that’s the reason Microsoft, CVS, Walgreens, Apple, Google, Healthways, Uber and others see huge opportunities to deliver more value to healthcare consumers.
Defining value in healthcare through the lens of the consumer is arguably more important than any other perspective. But it’s likely to remain healthcare’s most elusive term until consumers see it clearly by our actions.
Paul H. Keckley is Managing Director of the Navigant Center for Healthcare Research and Policy Analysis where he leads a team of analysts in assessing industry issues and regulations relevant to hospitals, medical groups, health insurers, drug and device manufacturers and policymakers at the state and federal levels.
No comments:
Post a Comment