By JEFF GOLDSMITH
 What to do about the seemingly inexorable rise in health spending has been the central health policy challenge for two generations of health economists and policymakers. In 1965, before Medicare and Medicaid, health spending was about 5.8 percent of GDP. In 2013, it was nearly 18 percent. And GDPquadrupled during this same period.
What to do about the seemingly inexorable rise in health spending has been the central health policy challenge for two generations of health economists and policymakers. In 1965, before Medicare and Medicaid, health spending was about 5.8 percent of GDP. In 2013, it was nearly 18 percent. And GDPquadrupled during this same period.
Over the past 30 years, there are been two warring political narratives explaining health spending growth, with two different culprits and indicated remedies. At their cores, these narratives blame the main actors in the health care drama—patients and physicians—for rising costs.
The Conservative Narrative: The Patient As Culprit
The conservative thesis holds that the demand for health care is unlimited because it has been, historically, a free good for many patients. Moreover, the argument runs, much illness is driven by bad personal health choices — for example, smoking and obesity, and the heart disease and diabetes that follows. Thus, much of our cost problem is actually the patient’s fault.
Since patients have historically paid a relatively small fraction of health costs, the conservative remedy is that patients must have more “skin in the game,” that is, pay more of the cost themselves. If we do this, people will exercise more discipline in their personal health habits, and also “shop” for care when they need to use it, and costs will go down.
Adherents to this explanation point to Joseph Newhouse’s nearly forty-year-old RAND health insurance study which showed that patients who shared some of the cost used a lot less care and were, apparently, no sicker at the end of the study period. The oft-ignored coda to the Rand study was that patients were incapable to distinguishing high-value from no-value care, a finding echoed just last week by a study of patient behavior in a high-deductible health plan.
This thesis — that lifestyle and indiscriminate use of care are the main drivers of heath spending — has led to multiple remedies: health savings accounts; higher cost sharing; higher patient front-end cash payments to doctors and hospitals; and also “price transparency” — attempting to clarify in advance of care what something will cost, so patients can use their own money to shop for care.
The conservative narrative had an influential role in shaping the structure of private coverage under the Affordable Care Act, where very high deductibles and annual out-of-pocket limits are the norm, as well as the Cadillac Tax on so-called “high value” health plans, designed to discourage first dollar coverage. It has led to a quintupling of patients with high deductible plans since 2007. According to the 2015 Kaiser Family Foundation Health Benefits Survey, patient cost sharing has grown six times as fast as wages since 2010.
The Progressive Narrative: The Physician As Culprit
The “progressive” narrative is more convoluted and absolves the patient of blame. The progressives’ culprit is the way we have traditionally paid for care: fee-for-service payment of doctors and per-admission or per-procedure payment of hospitals. Progressives, and many in the health policy community, believe that cost growth is actually driven by doctors and hospitals seeking higher incomes. The piecework incentive encourages hospitals and doctors to over treat or renders care that is completely unnecessary.
Physicians, it has been argued, have target incomes; to reach those targets, they will induce demand for care, e.g. find things to do to us solely to generate income. Reform advocates argue that if we change incentives to doctors and hospitals and compel providers to emphasize prevention and more effective care (paying for “value instead of volume”), costs will fall.
The behaviorist model of physician behavior has led to so-called “value-based payment” and the Physician (PQRS). This model has also now led to MIPS, the payment incentive model embedded in the 2015 Sustainable Growth Rate physician payment fix.
The core belief seems to be that if we can find the right “operant conditioning schedule” (per behavioral psychologist BF Skinner), physicians will do higher value works at lower patient risk. The result has been a regime of “micro-accountability”: astonishing increases in clinician reporting requirements from Medicare and commercial payers, and in the amount of time caregivers spend typing information into the patient’s health record in order to get paid. It has resulted as well in vast consulting and information technology outlays by providers to support new, highly complex payment approaches like the Accountable Care Organization and the Patient Centered Medical Home.
Dissecting The Narratives
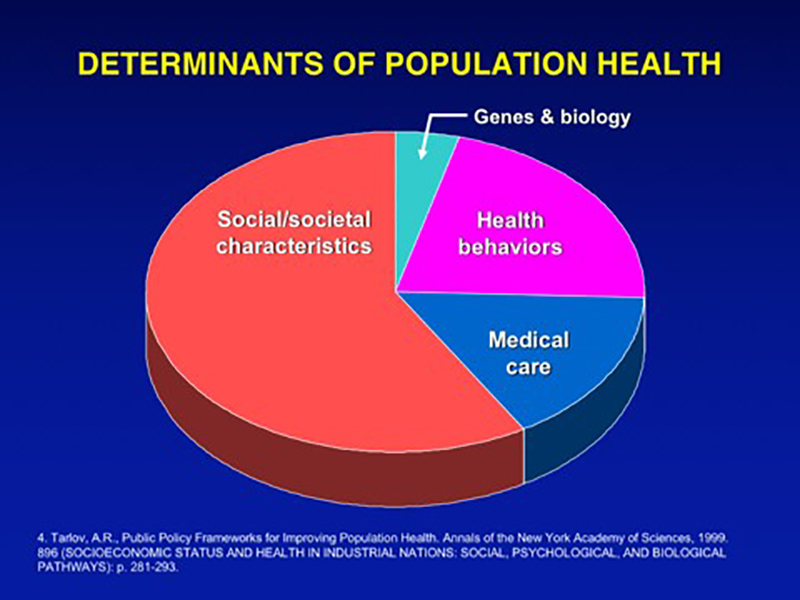
Problems with the conservative perspective: ignoring social factors. There are significant problems with both these narratives. On the conservative side, it is true that some behavioral issues, notably obesity and smoking, have major health cost consequences. As the graphic indicates, however, health behaviors account for a minority of health costs. It is laughable to think that minute or even significant economic incentives to the patient will negate the health effects of social determinants (poverty, lack of education, unemployment, compromised access to care), or of hundreds of billions spent advertising cigarettes, fast food, alcohol, and sugary snacks, or for that matter or of flawed “official” nutritional advice — let alone the accumulating effect of chronic disease as we age.
Exhibit 1
Reversing these problems is fundamentally a public health and political challenge that requires a multi-faceted approach with a lengthy, uncertain payoff. As we have seen with the sharp fall in adult smoking rates, and more recently, the accelerating decline in soft drink sales, progress is possible even if maddeningly slow to manifest itself.
The US significantly trails most OECD countries (to whose health systems ours is often unfavorably compared) in social spending. There has also been a lagging and inconsistent investment in public health in the US, despite the coverage gains from the Affordable Care Act.
To improve peoples’ health involves not only more consistent public health and social investment, but also a more just society and a more vibrant economy. In other words, improving health requires changing the society itself, not merely changing individual behaviors. There is clearly a piece of avoidable health care demand attached to changeable behaviors, but it is a lot smaller than its advocates believe.
Problems with the progressive approach: the explanatory limits of physician income maximization. On the progressive side, it is inconveniently the case that most of the countries to whom our US system is unfavorably compared (Switzerland, France, Germany, Canada) pay their hospitals and physicians on a piecework basis pretty much the same way we do, albeit with macroeconomic caps on total spending (e.g. global budgets). My spies in these countries tell me that their physicians do tend toward growing their incomes, but within definable, politically enforced limits.
But even inside the US, the “physician income maximization” hypothesis doesn’t explain why we have physician communities as diverse as Grand Rapids, Michigan, the two Portlands (Maine and Oregon), and Richmond, Virginia, where aggregate spending per capita for both Medicare and commercially insured patients is much lower than in most of the sunbelt or the northeast. Medicare’s payment methods are identical in all these places, and yet some physician communities practice a fundamentally more conservative style of medicine.
But most inconveniently of all, the income maximization hypothesis does not explain the sudden and sustained slowdown in spending we’ve experienced since 2008, with health spending growth subsiding to less than 4 percent annually. Health spending hasn’t grown this slowly in 50 years, since before Medicare and Medicaid, and spending has persisted at low levels seven years into an economic recovery.
Exhibit 2
Though there has been a recent modest uptick in health spending growth, core costs (e.g. hospital and physician services) have continued growing at pre-Medicare levels through 2014 and 2015 according to recent from the Centers for Medicare and Medicaid Services (CMS). The biggest outliers in the recent cost breakout: a single expensive new drug, Sovaldi, and sharp upticks in the cost of government administrative expense and the “net cost of health insurance” — both factors linked to implementing the Affordable Care Act.
The physician income maximization hypothesis also fails to explain the loss of 200 million physician visits since 2009, according to IMS Health. Did the irresistible lure of an open cash register suddenly end in 2009? Or, are other, more powerful forces at work, such as the retirement of activist baby boomer docs or the repricing of health services to the consumer due to the growth in high deductible plans? Only time and research inquiry will enable us to understand the reasons.
Progressives not only overestimate the effect of incentives on professional behavior. They also overestimate the capacity of the health system to improve the health of the population. Health care providers have negligible leverage to influence the social determinants of health or to significantly delay the onset of age-related chronic illnesses. Even with superb primary care infrastructure, the care system is a blunt instrument in improving the public health.
Health systems spend tens of billions every year in community benefit activities, many of which are targeted at community education, screening for controllable chronic diseases like heart disease and diabetes, sponsoring wellness activities that target increasing physical activity and improved nutrition, etc. This is all to the good.
But as long as health systems’ asset base and the bulk of their professional activities are devoted to caring for the sick and injured, acute care and mitigation of patient suffering will legitimately remain their core business.
Most care givers will never care as much for patients they are not seeing as the patients in front of them. Their fundamental moral and social obligation is to those immediately at risk for death or serious systemic injuries who have nowhere else to turn than the care system. Being complaint driven, the care system is inherently reactionary, as is any safety net.
Transcending The Two Narratives
On the other hand, there are big and reachable savings to be had for society and big benefits for their patients by eliminating wasteful use of resources when people do become ill, as well as by eliminating the iatrogenic causes of illness through improved safety and protocol-driven care. Health systems are striving to make more thoughtful use of the professionals who make up their operating core, by empowering them to continuously improve the care process. Care driven by evidence-based protocols, rather than inspired professional improvisation, can only help.
In the meantime, the twin demeaning narratives of moral failure—by individual patients according to conservatives and by caregivers according to progressives—continues to animate health policy and drive us toward simplistic marginalist economics solutions that reduce physicians and patients to merely economic actors.
The real story of what creates health and drives health spending is far more complex than these cartoon narratives suggest.
We need a more complex and balanced explanation of what creates health, and a more comprehensive set of solutions that implicate public health and the human services, as well as individual citizens and the care system. The care system by itself cannot improve Americans’ health.
Jeff Goldsmith, Ph.D., is the president of Health Futures Inc. and associate professor of public health sciences at the University of Virginia, Charlottesville.